Rhegmatogenous Retinal Detachment
Background
 The retina is the thin layer of tissue that retains the vision cells in the back of the eye. The retina is like the film inside a camera. The image that one sees is focused by the lens and cornea in the front of the eye and then cast upon the center of the retina (macula) in the back of the eye.
The retina is the thin layer of tissue that retains the vision cells in the back of the eye. The retina is like the film inside a camera. The image that one sees is focused by the lens and cornea in the front of the eye and then cast upon the center of the retina (macula) in the back of the eye.
A retinal detachment is a separation of the retina from the underlying layers of the eye wall. This will lead to progressive loss of peripheral and, eventually, central vision. Left untreated, total, permanent loss of sight eventually occurs in most cases.
Causes and Associations
A rhegmatogenous type of retinal detachment is caused by a break, tear or hole in the retina, allowing fluids from the vitreous cavity of the eye to track under the retina and detach it from the eye wall. “Rhegma” is Greek for rent or break. Rhegmatogenous retinal detachment is the most common type or retinal detachment.
Retinal tears and associated detachments of the retina are usually spontaneous events and cannot be predicted. It is caused by the vitreous gel separating from the retina. Over time as one grows older, the vitreous gel liquefies. It eventually collapses upon itself and separates from the surface of the retina. During or shortly after this event, a retinal tear can occur by the gel pulling on the retina.
Risk factors for developing retinal tears and detachment include myopia (near-sightedness), thin patches of the peripheral retina (lattice degeneration), previous eye surgery, and trauma.
Symptoms
Patients with rhegmatogenous retinal detachments often notice the sudden onset of floaters (black dots or cobwebs in their vision) and/or flashing lights. (These symptoms usually reflect the vitreous gel separation and retinal tear event.) A shadow, curtain, or cloud progressing from one’s peripheral vision comes next and this corresponds to the retina detaching. The rate of progression of the retinal detachment can vary from days to weeks depending on many factors such as patient age and size and number of retinal tears.
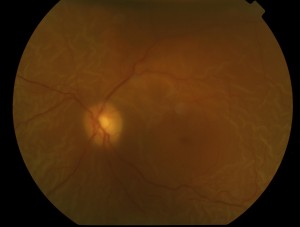
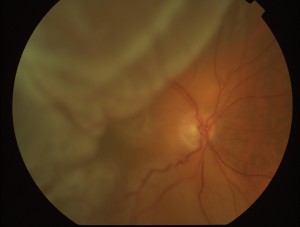
Examination
A comprehensive ophthalmic examination is essential to diagnose and treat a retinal detachment. Through a dilated pupil, the ophthalmologist will see one or more tears in the retina with varying amounts of underlying fluid. There may also be some degree of vitreous hemorrhage. (Hemorrhage is common when the retina tears.)
Prognosis
 Retinal detachments often cause some degree of permanent visual field or central visual acuity loss, even after successful retinal reattachment. Final visual outcomes are best if the detachment is detected and treated before it involves the center of the retina (macula). Longstanding retinal detachments typically have a poor visual prognosis. A change of glasses after healing from retinal detachment surgery may or may not improve the vision.
Retinal detachments often cause some degree of permanent visual field or central visual acuity loss, even after successful retinal reattachment. Final visual outcomes are best if the detachment is detected and treated before it involves the center of the retina (macula). Longstanding retinal detachments typically have a poor visual prognosis. A change of glasses after healing from retinal detachment surgery may or may not improve the vision.
Prevention and Treatment
If a retinal break or tear is detected before there is retinal detachment, laser or cryotherapy (freezing) to the retinal tear is often successful in sealing the tear and preventing a retinal detachment. However, once the retinal detachment develops, a retinal reattachment procedure is typically necessary.
There are three basic surgical procedures used to treat a retinal detachment. The choice depends on certain features of the detachment such as number and location of retinal tears among others.
Pneumatic Retinopexy is an office-based procedure. It involves injecting a temporary gas bubble to flatten (reattach) retinal tear and surrounding detachment. The gas injection is coupled with either a freezing treatment (cryotherapy) or laser photocoagulation to permanently seal the causative retinal tear. After the procedure, patients must maintain a certain head position for about 1 week to ensure the gas bubble properly closes the retina tear.
A Scleral Buckle Procedure is performed in the operating room. It consists of suturing a soft piece of silicone on the eye wall in such a way as to indent and close the retinal tear. It also is coupled with cryotherapy or laser photocoagulation. A gas bubble is also sometimes used during the procedure.
A Vitrectomy is another approach to reattach a retina and is also performed in the operating room. As the name implies, it involves surgical removal of the vitreous gel which, in turn, relieves the traction or pulling on the retinal tear causing the detachment. Like the other procedures, laser is used to seal the retinal breaks. At the end of this procedure, the eye is filled with either gas or silicone oil. Gas goes away slowly on its own, but oil is permanent and needs to be removed later with another operation. (The use of silicone oil is usually reserved for very complicated retinal detachments such as those associated with scar tissue.)